
知っていますか?Did you know about MKC?
ウェットフィールドアイWet Field Eye

こんな症状が出たら注意Watch for These Symptoms
土や水が目に入った後、次のような症状が出ていませんか?After soil or water gets into your eye, do you have any of the following symptoms?
- 目が赤い(充血)Red eye (bloodshot)
- 目がかゆい、ゴロゴロする、痛いItching, a gritty/foreign-body sensation, or pain
- 光をまぶしく感じるSensitivity to light (glare)
- 目が見えにくい、視界がかすむDifficulty seeing or blurred vision
どんな病気?What Kind of Disease Is It?
微胞子虫角結膜炎(ウェットフィールドアイ)は、微胞子虫という非常に小さな病原体が、目の表面(角膜・結膜)に感染し、炎症を起こす病気です。Microsporidial keratoconjunctivitis (MKC) is a disease in which a very small pathogen called Microsporidia infects the surface of the eye (the cornea and conjunctiva) and causes inflammation.
特にぬかるんだグラウンドや湿った芝生で、土や水が目に入ることで感染するといわれています。It is thought to be contracted when soil or water enters the eye, especially on muddy ground or wet grass.
サッカーやラグビーなど、土や水がかかりやすい屋外スポーツをする方に多く見られます。It is most often seen in people who play outdoor sports where soil and water easily get into the eyes, such as soccer or rugby.
蒸し暑い時期に、雨がたくさんふった後にプレーをすると、感染しやすいといわれています。Infection is said to be more likely if you play after heavy rain during hot, humid periods.
人から人へうつる(感染が広がる)ことは、今のところ確認されていません。Person-to-person transmission (spread of infection) has not been confirmed so far.
早めに適切な治療を受ければ、多くの場合は数週間で改善し、視力も回復します。With prompt, appropriate treatment, most cases improve within a few weeks and vision recovers.
最近の状況Recent Situation
以前からインドや東南アジアでは、集団発生が報告されています。Outbreaks have long been reported in India and Southeast Asia.

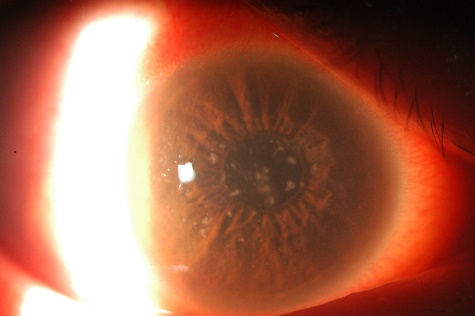
Mohanty A, et al. Ocul Surf. 2023 (Photograph of a patient infected in India)
Mohanty A, et al. Ocul Surf. 2023
- 2026年にはオーストラリアでフットボール選手約100人の集団発生が報告されました。In 2026, an outbreak affecting about 100 football players was reported in Australia.
- 日本国内でも、2022年以降、長崎県や神奈川県のサッカーチームやラグビーチームなどで集団発生が起こっています。ゴルフ選手の感染例も報告されています。In Japan as well, outbreaks have occurred since 2022 in soccer and rugby teams in Nagasaki and Kanagawa Prefectures. Cases in golfers have also been reported.
屋外スポーツをされる方は、誰にでも起こりうる病気として知っておくことが大切です。If you play outdoor sports, it is important to know that this disease can affect anyone.
こんなときは早めに眼科を受診してくださいSee an Eye Doctor Promptly If…
- 土や水が入った後、上記のような症状が続いているSymptoms like those above persist after soil or water got into your eye
- 症状が悪化している、または市販の目薬を使っても改善しないSymptoms are worsening, or do not improve even with over-the-counter eye drops
- 見え方が悪くなってきたYour vision has been getting worse
受診の際は、「サッカー・ラグビー・ゴルフなど屋外スポーツをしていて、グラウンドの土や水が目に入ったかもしれない」ということを、医師にお伝えください。診断や治療の参考になります。When you visit, please tell the doctor that you play outdoor sports such as soccer, rugby, or golf, and that soil or water from the ground may have gotten into your eye. This helps with diagnosis and treatment.
予防のポイントPrevention Tips
- プレー中に土や水が目に入った場合は、清潔な水でよく洗い流しましょう。If soil or water gets into your eye during play, rinse it well with clean water.
- 洗った後は清潔なタオルやティッシュで拭き、タオルの共用は避けましょう。After rinsing, wipe with a clean towel or tissue, and avoid sharing towels.
- コンタクトレンズを使用している方は、特に手洗い・レンズの衛生管理を心がけましょう。If you wear contact lenses, pay particular attention to hand washing and lens hygiene.
- 目に違和感が残る場合は、こすらずに早めに眼科を受診しましょう。If discomfort remains in your eye, do not rub it—see an eye doctor promptly.
国内・海外における集団発生の動向と臨床的留意点 Trends in domestic and overseas outbreaks, and clinical considerations
1.はじめにIntroduction
微胞子虫(Microsporidia)は、真菌に近縁の微生物で、様々な動物やヒトの細胞内に寄生し、主に免疫不全者に下痢・気管支炎などを引き起こす日和見病原体です。種によっては健常者においても微胞子虫角結膜炎(Microsporidial keratoconjunctivitis: MKC)を引き起こすことがあり、これまでインド・シンガポール・台湾・香港などの地域から集団発生が報告されています1,2)。近年、非流行地域であった日本やオーストラリアにおいて、屋外スポーツ選手を中心にMKCの集団発生が複数報告されており3-6)、本資料ではこれらの事例をもとに、参考情報を提供します。 Microsporidia are microorganisms closely related to fungi that parasitize the cells of various animals and humans. They are opportunistic pathogens that mainly cause diarrhea and bronchitis in immunocompromised hosts. Depending on the species, they can also cause keratoconjunctivitis (Microsporidial keratoconjunctivitis: MKC) in immunocompetent individuals, and outbreaks have been reported from regions such as India, Singapore, Taiwan, and Hong Kong1,2). Recently, multiple MKC outbreaks—mainly among outdoor-sports athletes—have been reported in Japan and Australia, regions previously considered non-endemic3-6). This material provides reference information based on these cases.
2.病態・臨床像の概要Overview of Pathophysiology and Clinical Features
- 感染経路Route
- 汚染された土壌・水との接触(ぬかるんだグラウンド、湿った芝のグラウンド、温泉、プール等)が主なリスク因子。二次感染(ヒト-ヒト感染)の証拠は確認されていない。Contact with contaminated soil or water (muddy ground, wet grass fields, hot springs, swimming pools, etc.) is the main risk factor. No evidence of secondary (human-to-human) transmission has been confirmed.
- 好発At-risk
- 屋外スポーツ選手(サッカー・ラグビー・ゴルフ等)、農業従事者、温泉利用者等。Outdoor-sports athletes (soccer, rugby, golf, etc.), agricultural workers, hot-spring users, and others.
- 症状Symptoms
- 片眼または両眼の結膜充血、かゆみ、光過敏(羞明)、視力低下、異物感・疼痛。Conjunctival hyperemia in one or both eyes, itching, photophobia, decreased visual acuity, foreign-body sensation, and pain.
- 所見Findings
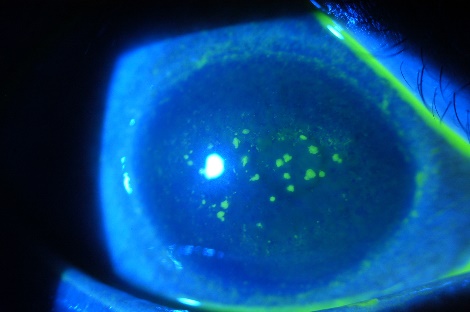
- 結膜充血および、角膜上皮に散在しフルオレセインで染色される顆粒状浸潤(図1)。Conjunctival hyperemia and granular infiltrates scattered in the corneal epithelium that stain with fluorescein (Fig. 1).

- 診断Diagnosis
- 問診と特徴的な前眼部所見で診断可能。確定診断には、角膜上皮擦過検体の塗抹検鏡やPCR検査が有用。塗抹検鏡では Calcofluor White、modified trichrome(chromotrope 2R)、抗酸菌染色(modified Ziehl-Neelsen)などの染色を用いる。Diagnosis is possible from the history and characteristic anterior-segment findings. For definitive diagnosis, smear microscopy of corneal epithelial scrapings and PCR are useful. Useful stains include Calcofluor White, modified trichrome (chromotrope 2R), and modified Ziehl-Neelsen (acid-fast).
- 治療Treatment
- 抗菌薬(フルオロキノロン系等)・抗真菌薬・消毒薬(PHMB・クロルヘキシジン等)の点眼や、角膜上皮擦過(実質へ移行しないよう愛護的に)が用いられる。ただし高いエビデンスレベルで確立した治療はない。Topical antibacterials (e.g., fluoroquinolones), antifungals, and antiseptics (e.g., PHMB, chlorhexidine), as well as gentle corneal epithelial debridement (avoiding extension into the stroma), are used. However, no high-level-evidence treatment has been established.
- 経過Course
- 多くは数週間以内に改善し、視力予後は良好。経過中に角膜上皮下浸潤を生じ、羞明が遷延する場合もある7)。ステロイド点眼は、感染が制御され、角膜上皮下浸潤が残存する際に慎重に投与する。Most cases improve within a few weeks, with a good visual prognosis. Subepithelial infiltrates (SEI) may develop during the course, with prolonged photophobia7). Topical steroids should be used cautiously once the infection is controlled and SEI persist.
3.集団発生の事例Reported Outbreaks
3-1. 長崎県(2022~2023年)3-1. Nagasaki Prefecture (2022–2023)3,4)
- 2022、2023年の7~10月、2つのサッカーチームにおける計16例の集団発生。A total of 16 cases across two soccer teams from July to October in 2022 and 2023.
- 多くの症例が、降雨後の高温多湿のグラウンドで、泥や水が眼に入った後に発症。Most cases developed after mud or water entered the eye on hot, humid ground following rainfall.
- 点眼治療や角膜上皮擦過で数週間以内に改善し、矯正視力0.1〜1.2から1.0以上に改善。With topical treatment and corneal epithelial debridement, cases improved within a few weeks; corrected visual acuity improved from 0.1–1.2 to 1.0 or better.
- PCRにより角膜上皮とグラウンドからMKCの原因となる微胞子虫(Vittaforma corneae)を検出。PCR detected the Microsporidia responsible for MKC (Vittaforma corneae) in both the corneal epithelium and the ground.
3-2. 神奈川県(2024年)3-2. Kanagawa Prefecture (2024)5)
- 2024年7~9月、同一サッカーチームにおける8例8眼の集団発生。An outbreak of 8 cases (8 eyes) in a single soccer team from July to September 2024.
- 角膜擦過とフルオロキノロン系抗菌点眼薬で全例4週間以内に改善し、視力低下例はなし。With corneal debridement and topical fluoroquinolone antibacterials, all cases improved within 4 weeks, with no cases of decreased visual acuity.
3-3. オーストラリア(2026年)3-3. Australia (2026)6)
- 2026年1月以降、複数チームのオーストラリアンフットボール選手約100例で集団発生。Since January 2026, an outbreak among about 100 Australian-rules football players across multiple teams.
- リスク因子は、ぬかるんだ・湿った競技場への暴露で、二次感染の証拠は確認されず。The risk factor was exposure to muddy, wet playing fields; no evidence of secondary transmission was found.
- 同州の保健省疾病対策センター(CDC)は、2026年3月に公衆衛生アラートを発行8)。The Northern Territory's Centre for Disease Control (CDC) issued a public health alert in March 20268).
参考文献・参考資料References
- Mohanty A, et al. Past, present, and prospects in microsporidial keratoconjunctivitis - A review. Ocul Surf. 2023. リンクLink
- 江口洋. 【私の経験集 珍しい真菌の角結膜感染への対応】マイクロスポリディア角結膜炎(解説). 眼科. 2023. Eguchi Hiroshi. Microsporidial keratoconjunctivitis (review). Ganka. 2023. (in Japanese)
- Uematsu M, et al. Microsporidial keratoconjunctivitis – first outbreak in Japan. BMC Infect Dis, 2023. リンクLink
- Mohamed MT, et al. Environmental and Climatic Drivers of Microsporidial Keratoconjunctivitis in Athletes: Molecular Evidence from Outbreaks in Japan. Microorganisms, 2026. リンクLink
- 柿栖康二ら. スポーツ選手に生じたMicrosporidia角膜炎の集団感染. 角膜カンファランス, 2025. Kakisu Kojo, et al. Outbreak of Microsporidia keratitis in athletes. Cornea Conference (Japan Cornea Society), 2025. (in Japanese)
- Powel S. Source of eye infection outbreak among 100 Darwin AFL players, Optometry Today, 2026. リンクLink
- 上松聖典ら. Microsporidia角結膜炎を繰り返し発症した1例. あたらしい眼科. 2026. Uematsu Masafumi, et al. A case of recurrent Microsporidial keratoconjunctivitis. Journal of the Eye (Atarashii Ganka). 2026. (in Japanese)
- Centre for Disease Control (Australia, NT Health). Public health alert: Microsporidial keratoconjunctivitis in AFL NT football players. 30 March 2026. リンクLink
文責: 長崎大学病院眼科 准教授 上松聖典Written by: Associate Professor Masafumi Uematsu, Department of Ophthalmology, Nagasaki University Hospital 2026年6月14日June 14, 2026